The incidence of Colorectal Cancer (CRC) continues to rise and currently CRC has become the second most common cancer in Malaysia (13.2%). The overall incidence rate for CRC was 21.3 cases per 100,000 population. Majority of patients are diagnosed at stage 3 and 4 (54.36%) while only 8.4% are diagnosed at stage 1. Surgical treatment of early CRC has proven to offer best curative outcome. Therefore, early detection of CRC is vital in order to reduce CRC-related deaths.
There is a 5-year survival rate of 90% when colorectal cancer is detected early, but because screening rates are low, less than 40% of colorectal cancers are found early. Early detection can greatly increase the chance of treatment being successful. Furthermore, CRC is potentially preventable if the tumour is detected at the precancerous stage, i.e colorectal polyps. Prevention of CRC is dependent upon early and regular screening to facilitate the detection and removal of precancerous colorectal polyps.
SCREENING
The following recommendations were highlighted in the Malaysian CPG of Management of CRC.
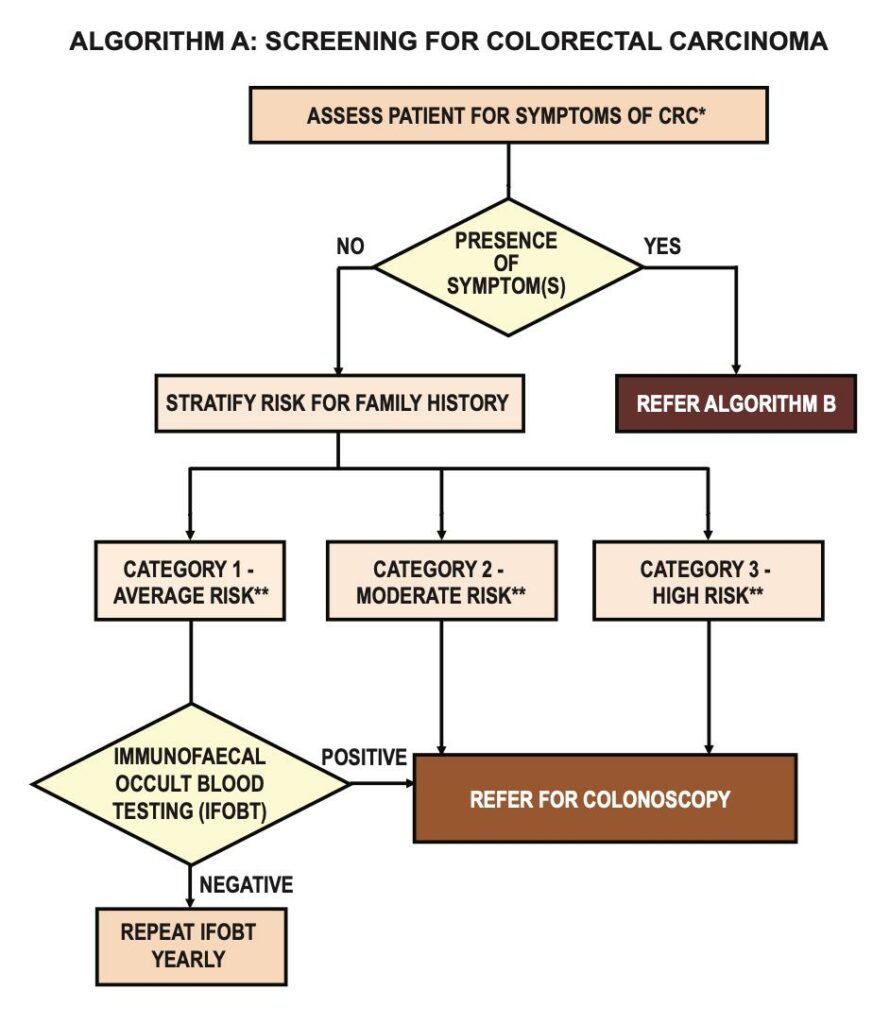
- Screening of CRC should be offered at the age of 50 years and continues until 75 years old for average risk population
- immunochemical faecal occult blood test (iFOBT) is the preferred method to screen for CRC in average risk population
- if iFOBT is positive, an early colonoscopy is necessary
- if iFOBT is negative, yearly test should be performed
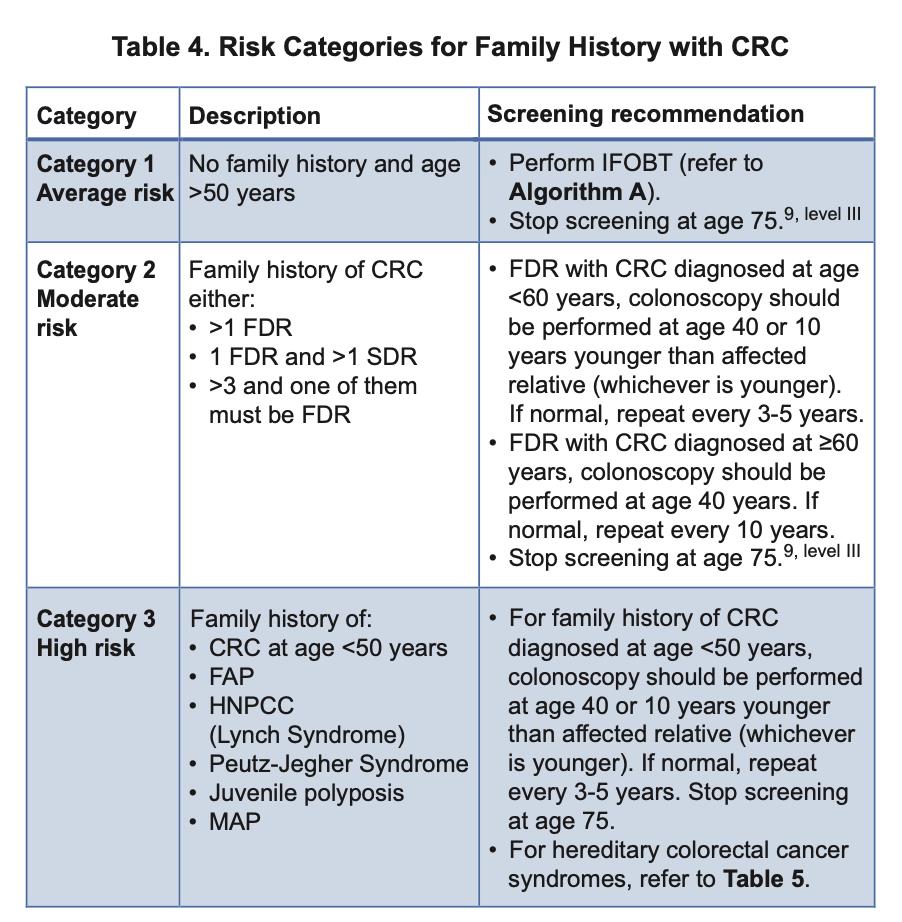
- However, if the individuals fall under the category of moderate or high risk, they should be directly referred for screening colonoscopy as early as at age 40 or 10 years younger than affected relative as illustrated in the table 4.
Most CRC arise from adenomatous polyps that progress from small to large polyps before transforming to cancer. The slow transition from polyps to cancers in most patients gives the window of opportunity for screening and cancer prevention by means of removal of the polyps. Colonoscopy is the most effective screening tool that has the ability to visualize the colonic mucosa directly, perform biopsy and excise the polyps.
Screening colonoscopy reduces overall CRC incidence significantly by 56% and death by 68% according to the literatures. For those who has had colonoscopy especially for screening, the risk of CRC is strongly reduced by 91% up to 10 years. Colonoscopy is a safe modality for colorectal screening in general population with low incidence of complication like GI bleeding or bowel perforation in experience hands.
RISK FACTORS
- Family history is a well-established risk factor for CRC. Those with positive family history of CRC will fall under the category of moderate or high risk depending on the degree of family relationship and the associated genes or hereditary CRC syndromes.
- Those with previous history of colon adenomatous polyps will carry higher risks to develop new polyps and CRC
- Patients with existing inflammatory bowel diseases like Ulcerative Colitis or Crohn’s Disease
- Smoking attributes to 16% greater risk of developing CRC compared with those who had never smoke
- Alcohol consumption greater than 30gm/day is positively associated with risk for CRC
- Excessive consumption of processed meat and red meat may be a risk factor for CRC based on current but limited evidence
- Patients with diabetes mellitus is found to have increased risk of CRC
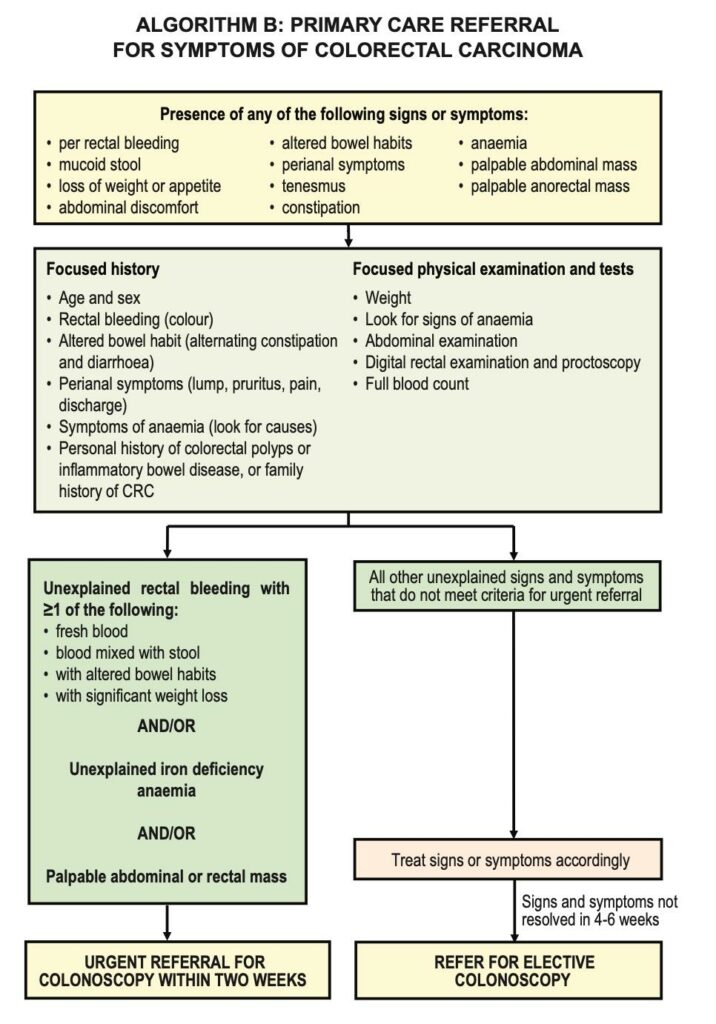
SYMPTOMS
The most common presenting symptoms of CRC are altered bowel habit (41.7%), followed by blood in stool (35.5%), abdominal pain (31.5%), weight loss (31%), anaemia (9.8%), and Intestinal obstruction (9.3%). It is vital to recognize the early symptoms like altered bowel habit for more than 2 weeks and not to wait until the late symptom of bowel obstruction.
TREATMENT
Surgery is the mainstay of treatment for CRC and offers the best curative outcome for localized disease. There are various modalities of surgical treatment, depending on the stages of the disease, tumour location in the colon/rectum, and the availability of the resources. Recent advances in minimally invasive and laparoscopic surgery have greatly improved the treatment outcome of the cancer. However advanced disease carries poor prognosis and frequently palliative in nature.
While surgery remained the primary treatment for CRC, chemotherapy, targeted therapy and radiotherapy are also playing important roles in CRC treatment as neoadjuvant, adjuvant and palliative options.
LAPAROSCOPIC OR MINIMAL INVASIVE COLORECTAL SURGERY